Ketogenic Diet and Cannabidiol Show Seizure Reduction in Drug-Resistant Epilepsy
A Johns Hopkins chart review suggests CBD and keto may stack seizure control, especially when CBD starts first. The data are retrospective, but the signal is real-world and clinically useful.
What this combination story asks families first
When ketogenic diet therapy and cannabidiol are both already on the table, the practical question is not whether each can matter on its own. It is whether layering them can buy more seizure control for people with drug-resistant epilepsy, especially when earlier therapies have already fallen short. A Johns Hopkins-linked chart review points to a cautious yes: in a real-world cohort, the combination was associated with meaningful seizure reduction, and the order of treatment may have influenced how well it worked.


That matters because drug-resistant epilepsy is not a casual label. It is generally used when sustained seizure control does not happen after two appropriately chosen, adequately administered, well-tolerated anti-seizure medications. For families living inside that definition, every additional option has to earn its place on both effectiveness and tolerability.
What the chart review actually found
The study, titled *Concurrent Use of Ketogenic Diet Therapy and Cannabidiol in Children*, looked back at 58 people who received both CBD and ketogenic diet therapy between 2018 and 2025. The cohort was unusually broad, stretching from infancy to 60 years old, with a median age of 2 years when the combination began. That makes it a window into a very young, medically complex population, even though adults were included too.
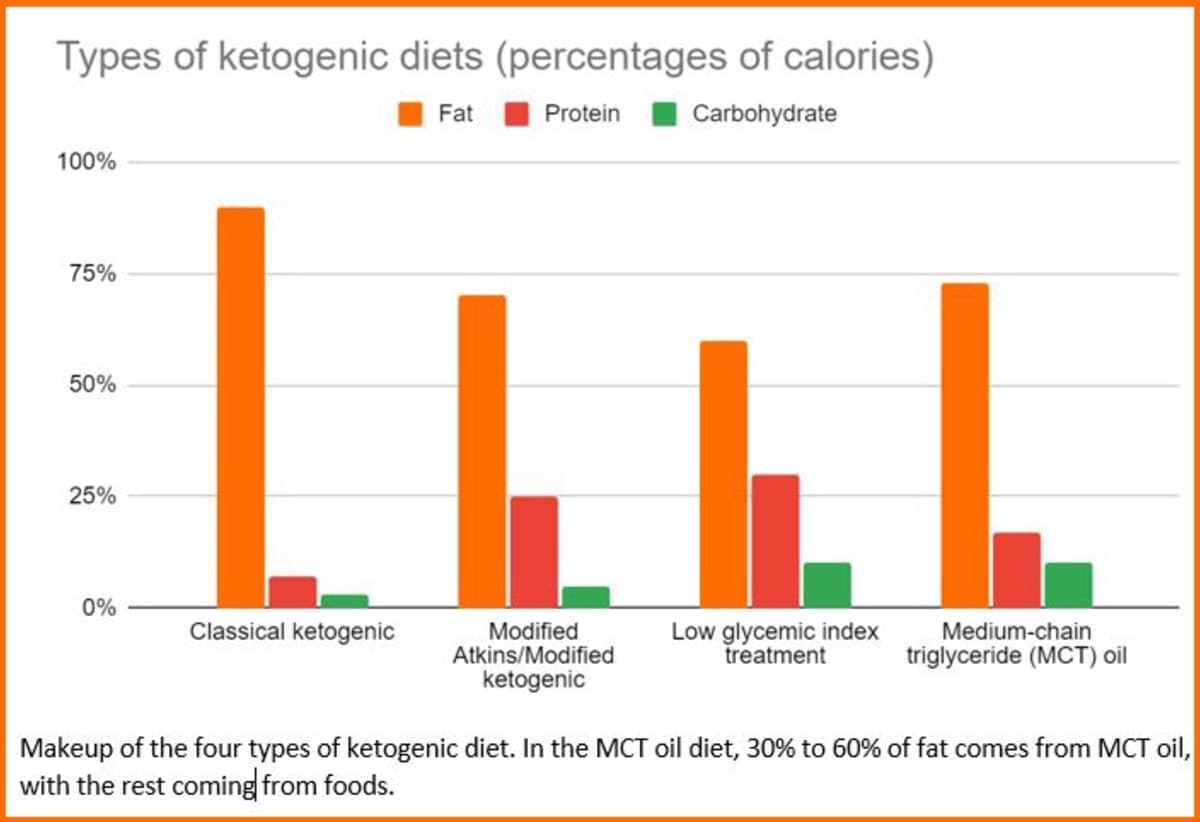
Most of the patients, 76%, were using prescription CBD sold as Epidiolex, while 24% used artisanal CBD. About 60% were on the classic ketogenic diet, the high-fat, very low-carbohydrate version many people think of first when they hear “keto for seizures.” The rest were using other ketogenic approaches, which fits the broader modern diet landscape that now includes classic ketogenic diet, modified Atkins, medium chain triglyceride diet, and low glycemic index treatment.
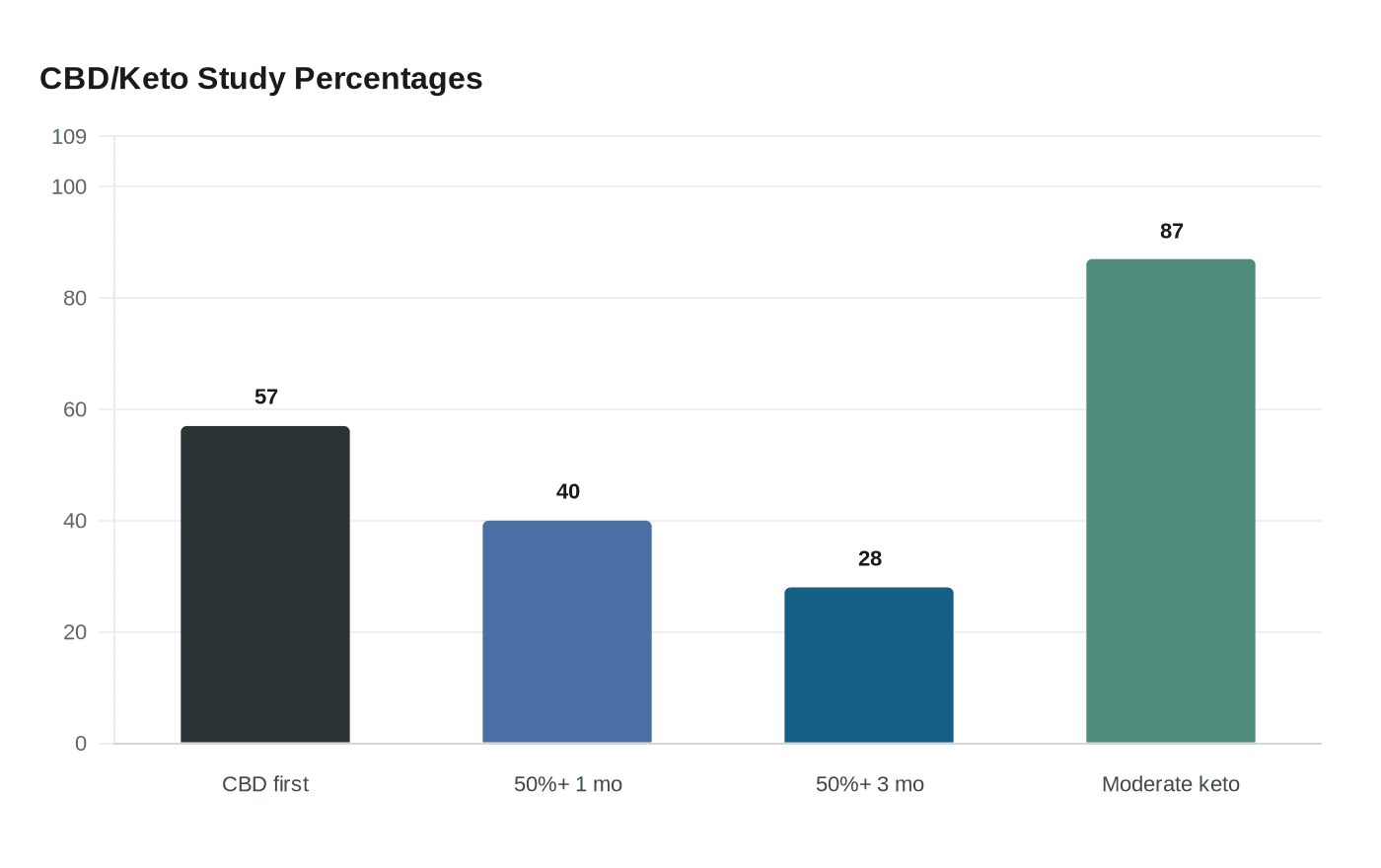
The seizure signal was the headline result. At one month, 40% of participants had more than a 50% reduction in seizures. At three months, 28% were still above that threshold. That is not a cure, and it is not proof of causation, but it is the kind of signal clinicians notice when families are running out of room to maneuver.
Why sequencing may matter
One of the most interesting details is timing. In this cohort, 57% of patients started CBD before they began ketogenic therapy. The researchers found that seizure reduction tended to be greater when CBD came first, then keto followed. That does not mean the reverse sequence cannot work, but it does suggest the order of introduction may shape the response.
For clinicians, that is a useful clue. It hints that these therapies may not simply overlap in a generic way, with each doing its own separate job. Instead, they may interact in a way that changes the overall seizure burden, which is exactly the kind of question a retrospective chart review can raise even if it cannot settle it.
What happened to ketosis and safety
One of the biggest practical concerns in the keto community is whether another therapy will disrupt ketosis. Here, the answer was reassuring. Urinary ketosis remained common, with 87% of participants reporting moderate to large ketosis. In the subgroup that added CBD to ketogenic therapy, most showed no major change in ketosis.
That matters because the ketogenic diet’s seizure benefit depends on consistency, monitoring, and adherence. Johns Hopkins has long emphasized that keto is not a casual self-experiment. The program there says its pediatric epilepsy team has nearly 100 years of experience, has treated more than 1,500 children, and helped develop the modified Atkins diet in 2002 before opening the world’s first adult epilepsy diet center. That kind of deep institutional history is exactly why a modern combination study like this draws attention: it is not just about an old therapy, but about how one of the field’s most established tools behaves when paired with a newer treatment.
The safety picture was manageable, but not empty. Five participants had increases in liver function tests on documented testing, though the paper characterizes most of those changes as minor. For families and clinicians, that is a reminder that even promising combinations still need the usual monitoring, especially when prescription CBD is part of the picture.
Why Johns Hopkins history gives this story weight
The ketogenic diet has been used continuously since 1921, and the International Ketogenic Diet Study Group has described ketogenic dietary therapies as established, effective nonpharmacologic treatments for intractable childhood epilepsy. That long track record gives this chart review a different kind of resonance. It is not introducing keto as a fringe idea. It is asking what happens when a century-old therapy meets a newer cannabinoid treatment in the same hard-to-treat population.
Johns Hopkins has been central to that story for decades. Its pediatric epilepsy team says it has almost 100 years of ketogenic experience, and Johns Hopkins materials note the program has treated seizures with the diet since the therapy’s origins in the 1920s. In that context, a Johns Hopkins-linked review of CBD plus keto is not just a curiosity. It is a sign that experienced epilepsy teams are still refining how to sequence and combine the tools they already trust.
What clinicians and families may take from it
The most important lesson is restraint paired with possibility. This study does not show that CBD plus ketogenic therapy is superior to either alone in a trial-proven sense. It does suggest that the combination can be used in real-world epilepsy care, that ketosis can be preserved in most patients, and that seizure reduction may be stronger when CBD is introduced before keto.
For families managing refractory epilepsy, that is meaningful because the decision is rarely about perfect evidence. It is about what can still be tried when the first two, three, or more therapies have not delivered sustained control. The chart review suggests that cannabidiol and ketogenic therapy are not mutually exclusive lanes. They may be additive, and in some patients, the sequence of the two may matter as much as the fact that both are being used.
That is not the end of the story. It is the part where clinical judgment, careful monitoring, and realistic expectations start doing the work that a retrospective study cannot do for them.
Every story on Keto Diet Magazine is assembled by an automated editorial system that works from verified research, official records, and credible reporting, then clears automated accuracy and moderation checks before it goes live. The standards that system follows are set and overseen by the people who run the publication. Read our full editorial policy.
Did this article answer your question?