From fringe diet to clinic
A long-standing patient’s turnaround can change a doctor’s thinking faster than any conference slide deck. That is the story McLean Hospital says pushed Chris Palmer toward ketogenic therapy in 2017, after he witnessed improvement in a patient with schizoaffective disorder. Since then, interest has widened from bipolar disorder into severe depression and anorexia, with clinical attention now following patient outcomes instead of dismissing them as outliers.

What makes this moment different is not just the excitement, but the kind of evidence driving it. The field is moving from individual case stories to pilot trials, randomized studies, and now a formal expert consensus on how ketogenic therapy should be defined, who may qualify, and how it should be monitored. That shift is why keto is starting to look less like a fringe experiment and more like a serious psychiatric intervention under study.
What the early data is actually showing
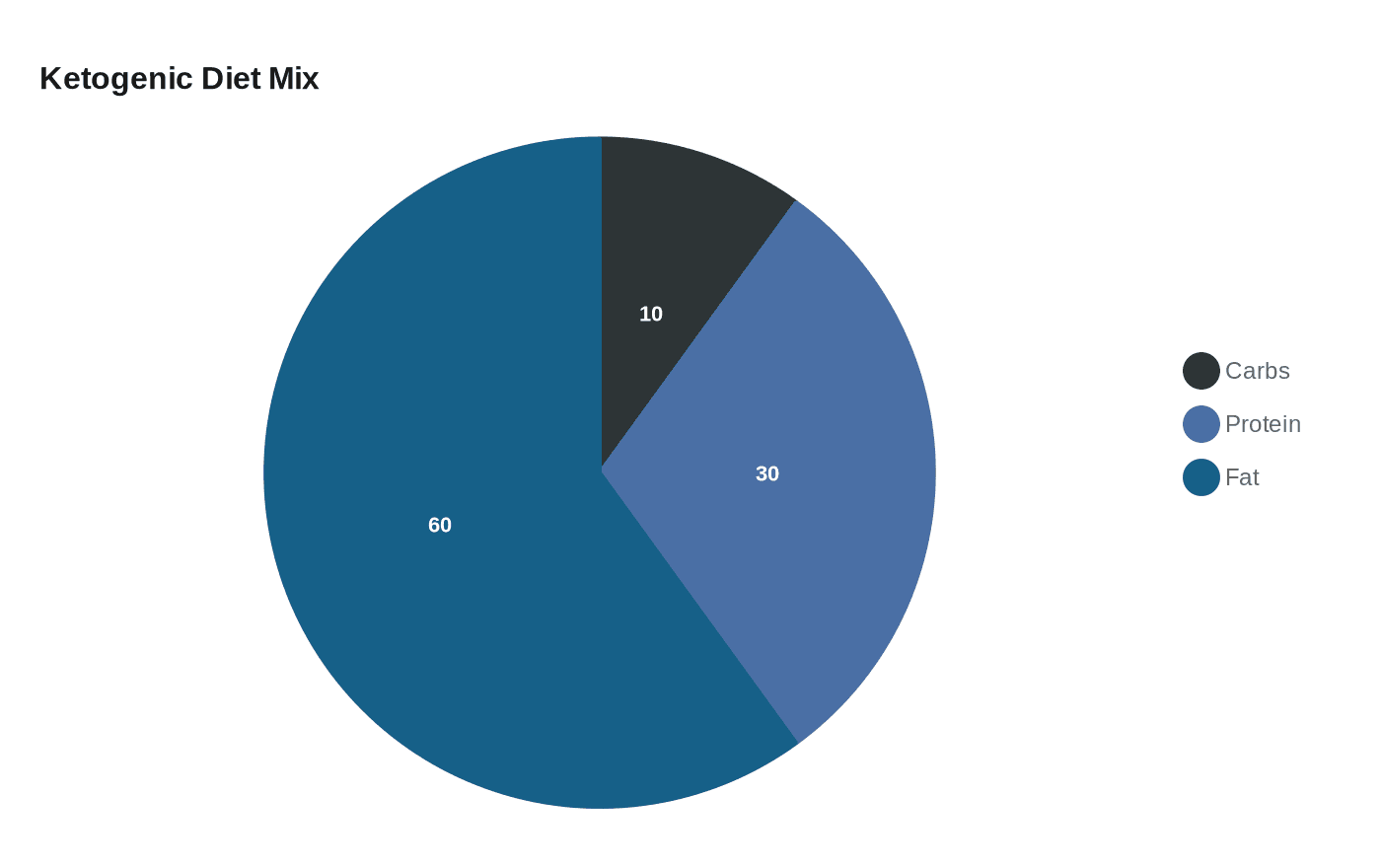
The clearest modern signal comes from Stanford Medicine’s pilot trial of 21 adults with schizophrenia or bipolar disorder and metabolic abnormalities. Led by psychiatrist and obesity specialist Shebani Sethi, the four-month study prescribed a ketogenic diet built around roughly 10% of calories from carbohydrates, 30% from protein, and 60% from fat. Stanford later summarized the results as showing about a 30% reduction in psychiatric symptoms and an average 10% weight reduction among participants who adhered.
That matters because the study population was not a generic keto crowd. These were adults already dealing with serious mental illness, metabolic problems, and antipsychotic treatment. In other words, the intervention was aimed at a medical overlap zone where brain symptoms and body metabolism seem to be tangled together. Stanford’s own framing was that the metabolic effects of keto may help stabilize the brain, which is a very different claim from using keto simply to drop scale weight.
The broader research literature is still early, but it is starting to stack up. A 2024 review in Springer said case reports and case series suggest ketone-based therapy may help bipolar disorder, and a Frontiers in Nutrition protocol laid out a randomized controlled trial of ketogenic metabolic therapy for schizophrenia and bipolar disorder. Put together, those pieces do not prove the case yet, but they do show a field trying to graduate from anecdote to design.
Why bipolar disorder is drawing so much attention
Bipolar disorder has become one of the clearest testing grounds because the signal appears in both clinic stories and structured studies. McLean Hospital says Palmer’s turning point in 2017 came after the response of a patient with schizoaffective disorder, and that experience helped push the hospital to launch a randomized controlled trial of ketogenic therapy for 50 people with early bipolar disorder. That design matters: it moves the question from “can this help one remarkable patient?” to “does it hold up across a group?”
The appeal is easy to understand if you follow the field’s logic. Bipolar disorder often intersects with metabolic issues, and the Stanford pilot specifically enrolled people with those abnormalities. For clinicians drawn to keto in this setting, the hope is that changing fuel availability may influence mood stability as well as weight and metabolic health. The caution is just as important: this is still an emerging treatment path, not a replacement for standard psychiatric care.
Depression and anorexia widen the conversation
Severe depression is now part of the conversation around keto, even as the strongest formal studies described here focus on bipolar disorder, schizophrenia, and anorexia. That widening interest is what gives the story its momentum. The same metabolic hypothesis that has pulled psychiatrists toward bipolar disorder is also attracting attention in mood disorders more broadly, especially where conventional treatment has left patients searching for another lever.
Anorexia is a different kind of test case altogether. UC San Diego’s trial, which began in October 2023 and is expected to run until around June 2027, is enrolling people ages 18 to 45 and includes both a weight-recovered cohort and an underweight sub-study. The study is asking whether therapeutic ketosis can reduce drive to restrict, body dissatisfaction, mood symptoms, and anxiety. That is a careful and ambitious question, because it treats anorexia not as a simple nutrition problem, but as a disorder where cognition, fear, and body image all collide.
The design also shows how differently clinical keto is being used here compared with hobbyist keto. In weight-loss circles, people often chase fat loss, appetite suppression, or blood-sugar control on their own terms. In anorexia research, the aim is not weight loss at all. It is whether a tightly supervised metabolic intervention can calm the mental machinery that keeps restriction locked in place.
What supervision looks like when keto becomes treatment
Clinical keto is not freestyle keto. The 2026 expert consensus published in Frontiers in Nutrition is the clearest sign that the field is trying to standardize practice. Built around 33 evidence-based statements, it covers definition, eligibility, monitoring, and best practices for ketogenic therapy in serious mental illness. That is the sort of framework clinicians need before they can make keto feel less like a bold idea and more like a reproducible protocol.
In practice, supervision means the diet is being used inside a medical structure, not as an internet challenge. Stanford’s trial involved adults with metabolic abnormalities who were already prescribed antipsychotic medications, and McLean’s trial is an outpatient randomized controlled study. Those details matter because psychiatric keto is being studied in people who need close follow-up, not self-experimentation.
The mixed reaction around the field reflects that tension. Some clinicians and researchers see a potentially transformative approach, especially when metabolic dysfunction and psychiatric symptoms overlap. Others stress that the evidence is still early-stage and that keto has to be judged against established psychiatric treatment, not marketed as a substitute for it.
The takeaway for the keto community
If you already know keto as a tool for weight loss, the psychiatric version will feel familiar on the macros and completely different in purpose. The attention now building around depression, bipolar disorder, and anorexia is being driven by structured trials, case reports, and a growing effort to define therapeutic ketosis as a real medical intervention. The most promising path appears to be narrow, supervised, and diagnosis-specific.
That is the big shift: keto is no longer being discussed only as a lifestyle choice. In serious mental illness, it is entering the clinic as a question of who may benefit, what level of oversight is required, and whether changing metabolism can genuinely change the brain.
Every story on Keto Diet Magazine is assembled by an automated editorial system that works from verified research, official records, and credible reporting, then clears automated accuracy and moderation checks before it goes live. The standards that system follows are set and overseen by the people who run the publication. Read our full editorial policy.
Did this article answer your question?