
Keto has always sold itself as a way to make weight loss feel more controlled, more intentional, and, ideally, less punishing on muscle. This small case series asks what happens when that logic meets semaglutide, one of the defining drugs of the GLP-1 era, and the early signal is encouraging enough to get attention. Most of the weight came off as fat, not lean tissue, but the study is still a sketch, not a verdict.
Why this pairing is getting attention
The reason clinicians keep circling back to this question is simple: GLP-1 drugs can drive impressive weight loss, but not all of that loss is purely fat. The paper notes that up to 40 percent of weight lost on GLP-1 receptor agonists may come from lean body mass, and that worry has only grown as semaglutide has become central to obesity care.
That concern is backed by a larger retrospective cohort published in JAMA Network Open on January 9, 2026. In that study of 3,066 patients, including 1,809 nonsurgical patients who started semaglutide or tirzepatide between November 12, 2018 and December 6, 2023, GLP-1 receptor agonists were linked to substantial fat mass loss and modest fat-free mass loss over 24 months. Bariatric surgery produced even more favorable fat-free-mass-to-fat-mass changes, which sharpened the question this keto study tried to answer: can diet composition help steer semaglutide’s weight loss toward fat?
What the case series actually tested
The report, by Genevieve Parker, Madeline D. Morris, Jeter R. Heggie, Ella F. Cooper-Leavitt, Cameron J. Clark, Asher P. Reynolds, Holly A. Smith, Carlie P. Wendel, William J. Jensen, Tyson J. Morris, Paul R. Reynolds, and Benjamin T. Bikman, came from Brigham Young University in Provo, Utah, Summit Family Health–Metabolic Clinic in Meridian, Idaho, and Creighton University School of Medicine in Phoenix, Arizona. It was submitted on April 21, revised and accepted on June 8, and published on June 12 in the Journal of Personalized Medicine as part of a Special Issue on Personalized Medicine of Obesity and Metabolic Disorders.
The study followed seven analyzed adults, six female and one male, with baseline BMI values ranging from 25.6 to 47.2 kg/m². They completed a clinician-supervised, six-month program built around a whole-food ketogenic diet plus semaglutide at 1.0 mg per week or less. That low-dose detail matters, because this was not a test of maximal drug exposure. It was a practical attempt to see whether a food-first low-carb pattern could work alongside a modest GLP-1 dose.
What changed over six months
The headline number is straightforward: mean total weight loss was 21.9 kilograms. More importantly for keto readers, about 92 percent of that loss was estimated to come from fat mass, which is the outcome people hope for when they trade carbs for ketones and appetite control for structure.
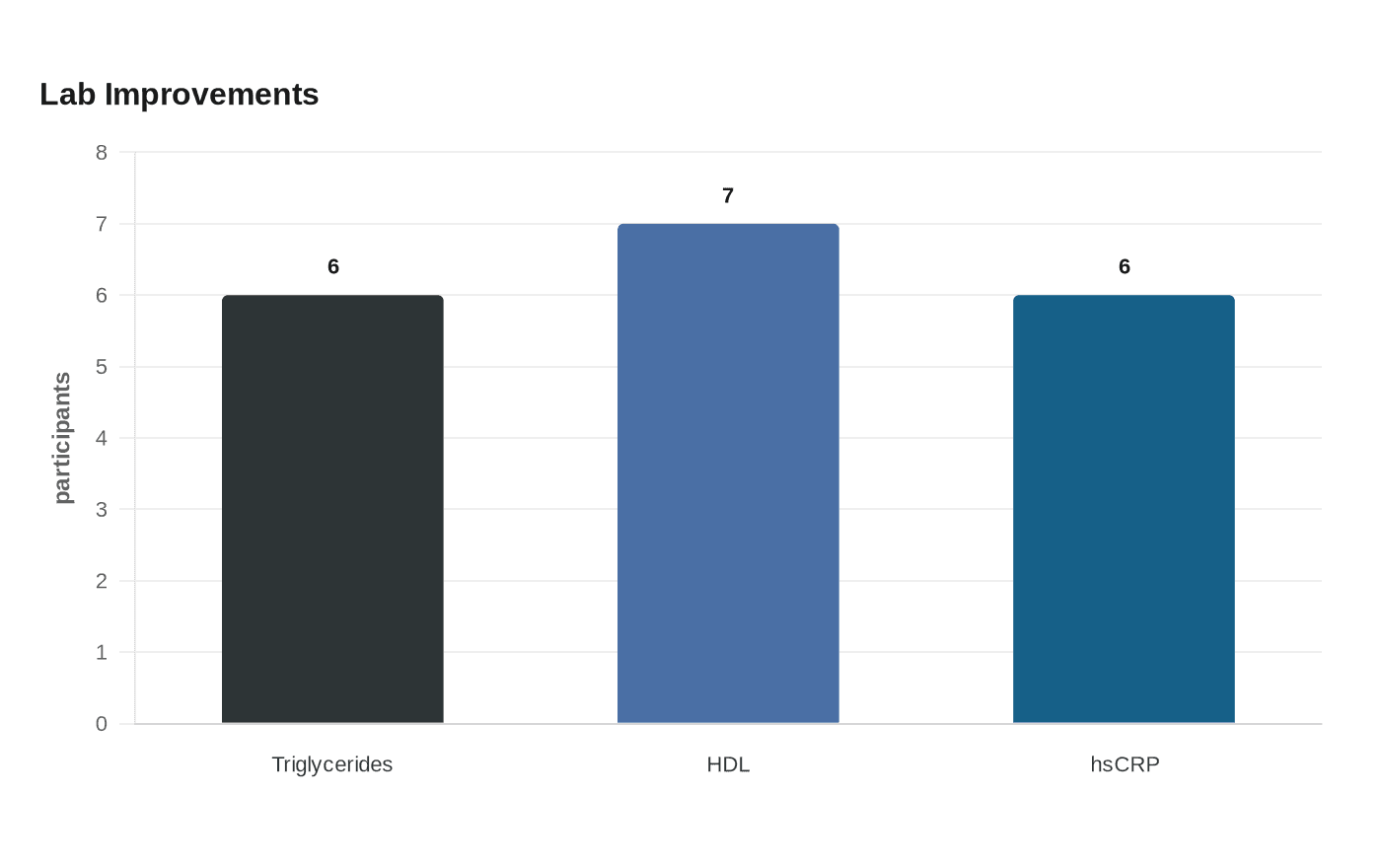
Lean tissue held up reasonably well. Mean skeletal muscle mass loss was 1.2 kilograms by bioelectrical impedance analysis, and one participant actually gained lean tissue. Metabolic markers improved alongside the scale drop, with fasting insulin falling by a mean of 15.6 µIU/mL and visceral fat decreasing by a mean of 37.0 percent. Triglycerides fell in six of seven participants, HDL cholesterol rose in all seven, and high-sensitivity C-reactive protein improved in six of seven. LDL cholesterol responses were mixed, which is exactly the kind of reminder keto readers already know well: the same approach can produce very different lipid results from one person to the next.
What to watch if you are thinking about the combo
This is the part of the story that deserves the most skepticism. Semaglutide can make it easier to eat less, but that can also make it easier to under-eat, especially if protein intake is not planned deliberately. On keto, where carbohydrate is already capped, the difference between a body-composition win and a lean-mass loss problem often comes down to enough protein, enough total intake, and enough consistency to keep the diet sustainable.
A few practical tradeoffs stand out:
- Appetite suppression can help adherence, but it can also make meals feel optional.
- Protein has to stay intentional, because low appetite can quietly crowd it out.
- GI side effects, which are common with GLP-1 therapy, can make a whole-food plan harder to maintain if meal size or fat tolerance drops.
- LDL can move in the wrong direction even when weight, insulin, and triglycerides improve.
- A whole-food ketogenic pattern is more plausible long term than a rigid macro chase built on highly processed keto products.
That last point matters because the study was not really about a hack. It was about whether a clinician-supervised, food-centered low-carb plan could help people stay on a path that protects muscle while semaglutide does the heavy lifting on appetite.
Why this is a starting signal, not proof
The authors are careful about the limits, and readers should be too. This was a small, retrospective case series with no control group, so it cannot prove that keto caused the favorable body-composition pattern or that semaglutide plus keto is superior to semaglutide alone. It also relied on bioelectrical impedance analysis, which is less definitive than DXA or MRI for measuring tissue composition.
That limitation does not make the paper uninteresting. It makes it useful in the right way: as a signal that deserves a better trial. The broader research picture is already moving in that direction, with reviews and ongoing studies focused on preserving lean mass during GLP-1 treatment, including work suggesting that co-administration strategies such as ketone ester may blunt semaglutide-related skeletal muscle loss without giving up fat loss. Semaglutide already has a strong track record in obesity trials, with one review noting about 15 percent initial weight loss at 68 weeks alongside cardiometabolic benefits, so the next question is not whether the drug works, but how to keep the loss where people want it.
For keto readers, that is the real tension in this story. Semaglutide may make the scale move faster, but keto still has to answer the harder question: can the loss stay mostly fat, keep enough muscle, and remain livable after the first burst of enthusiasm wears off?
Every story on Keto Diet Magazine is assembled by an automated editorial system that works from verified research, official records, and credible reporting, then clears automated accuracy and moderation checks before it goes live. The standards that system follows are set and overseen by the people who run the publication. Read our full editorial policy.
Did this article answer your question?


