Thousands of patients who hit a wall on strict low-carb and keto protocols broke through it, losing a full 20% of their body weight, after Dr. Spencer Nadolsky, a board-certified obesity and lipid specialist, shifted them onto GLP-1 medications paired with higher carbohydrate and lower fat intake. The result challenges one of keto's most deeply held assumptions: that dietary carbohydrates are the central obstacle to sustained fat loss.
The reason the classic carbs-vs-fat argument loses traction once a GLP-1 is in the picture comes down to brain chemistry. GLP-1 receptors in the brain profoundly influence satiety, so the hunger pressure that once made strict carbohydrate restriction a necessary behavioral guardrail gets quieted pharmacologically before the first meal of the day. Nadolsky and his colleagues have closely monitored a large patient population consisting of tens of thousands of individuals using GLP-1 agonists to address weight loss, giving him a clinical vantage point few obesity physicians can match. He now runs Vineyard, a physician-led virtual obesity clinic built around personalized GLP-1 care.
That clinical breadth, however, has never made Nadolsky a dietary ideologue. He openly explores low-carb nutrition, low-fat nutrition, and multiple forms of exercise, deploying each to help individual patients rather than defending any single protocol. Keto still earns its place for patients managing significant glycemic swings or prediabetes, where carbohydrate restriction reduces insulin spikes that appetite suppression alone cannot fully offset. But for patients on semaglutide or tirzepatide, GLP-1 agonists now induce an average weight loss of 15 to 20% of total body weight with a once-per-week injection, and adding carbohydrates rather than doubling down on dietary fat can reduce the friction and GI distress that derail long-term adherence.
The muscle preservation problem is where this gets urgent for the keto community. Lean soft tissue loss comprised 26% to 40% of total weight lost in recent GLP-1 trials, according to a 2025 case series co-authored by Nadolsky and body composition researcher Dr. Grant Tinsley. Their research seeks to help patients lose fat while maintaining muscle, with the goal of improving long-term health. The practical prescription that emerges from their work: hit protein targets in the range of 100 to 120 grams daily and anchor your week around resistance training. Vineyard's LiftRX program is built around exactly this principle. Nadolsky has observed that when patients reduce their GLP-1 dose and return to the gym, a significant number start breaking through plateaus that the medication alone could not crack.
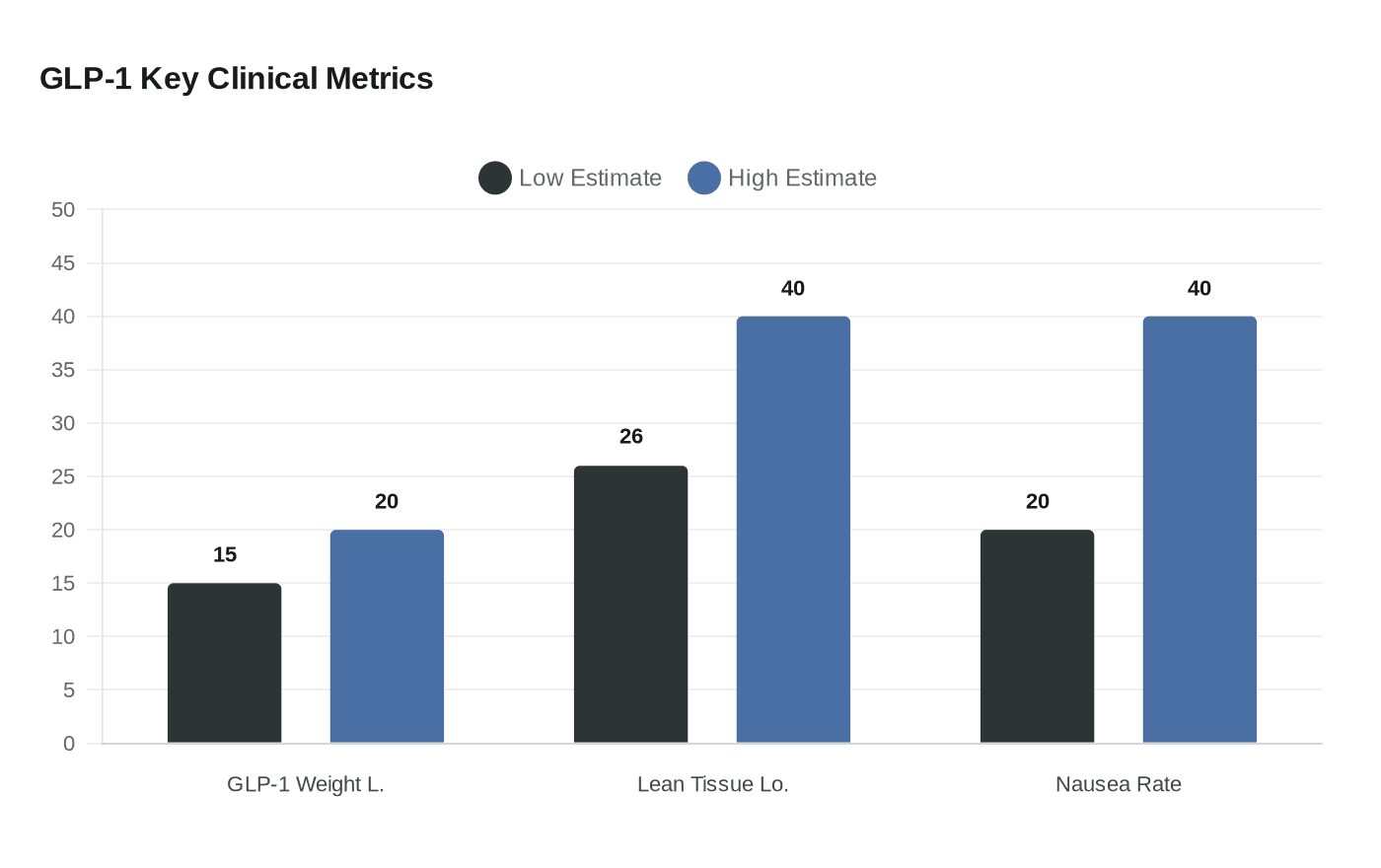
Reintroducing carbohydrates after a stint on keto requires patience, especially on a GLP-1. GLP-1 receptor agonists delay gastric emptying, contributing to enhanced satiety but also increasing nausea risk, and a sudden flood of refined carbohydrates compounds that risk considerably. Nausea is the most frequently reported adverse event among GLP-1 users, with rates ranging from 20% to 40% depending on the agent and dose. Gradual reintroduction using fiber-dense whole food sources, not white rice and bread, gives the gut time to adjust. Too much dietary fat independently worsens digestive issues on GLP-1 medications, so the high-fat approach that defined your keto phase can backfire once the medication is running.
Nadolsky's clinical argument, built across thousands of patients, is ultimately a personalization case: keto is a tool with a specific job, and once a GLP-1 is doing that job better, holding onto strict macros out of habit is just leaving results on the table.
Every story on Keto Diet Magazine is assembled by an automated editorial system that works from verified research, official records, and credible reporting, then clears automated accuracy and moderation checks before it goes live. The standards that system follows are set and overseen by the people who run the publication. Read our full editorial policy.
Did this article answer your question?