Fatty liver, spiking triglycerides, and stubborn visceral fat share a common upstream driver: too many refined carbohydrates overwhelming a liver that was never designed to process them at modern volumes. Dr. Sayajirao Gaikwad, who practices metabolic nutrition under the handle @DietDrsayajirao and works across homeopathy and dietary therapy, has made this the core of his clinical philosophy: "Obesity? Eat more proteins, restrict carbs. Fatty liver? Eat more proteins, restrict carbs. Diabetes? Eat more proteins, restrict carbs." His approach doesn't demand full ketosis. It demands precision, and the results from his patients suggest that precision is more than enough.
Why Keto-Adjacent Works When Strict Keto Doesn't Stick
The keto community already knows the fat-loss ceiling that carb restriction can unlock, but many people struggle to maintain ketosis long-term due to social eating, high cost, or adherence fatigue. The good news backed by clinical data: you don't need to stay below 20g of carbs daily to meaningfully reverse fatty liver and lower triglycerides. A carbohydrate-reduced, high-protein (CRHP) approach, one that simply shifts macros away from refined carbs and toward protein and fiber-dense vegetables, has been shown in a randomised controlled trial published in *Diabetologia* to improve HbA1c and liver fat content in weight-stable participants with type 2 diabetes over just six weeks. That's a moderate macronutrient shift, not a radical dietary overhaul, producing measurable liver changes.
Two weeks of dietary carbohydrate restriction reduced hepatic triglycerides by approximately 42% in subjects with nonalcoholic fatty liver disease (NAFLD), with reductions significantly greater than those achieved through calorie restriction alone. That single data point should reframe the way you think about what's driving liver fat accumulation: it's not excess calories in the abstract; it's specifically carbohydrate-driven lipogenesis, the liver converting surplus glucose into fat because it has nowhere else to put it.
The Plate Template: Build It Once, Reuse It Every Meal
Dr. Gaikwad's clinical plate draws directly from evidence-aligned nutrition principles and maps onto a repeatable structure you can deploy at lunch or dinner without recalculating macros every day. Here's the framework:
- Half the plate: non-starchy vegetables. Cooked low-GI vegetables combined with a raw salad component. Dr. Gaikwad specifically uses cucumber, carrot, and beetroot in raw form alongside cooked greens. This combination delivers high fiber and volume without triggering glucose spikes, while supporting gut microbiome diversity. The fiber slows gastric emptying, which is exactly what you want when managing post-meal blood sugar and liver fat accumulation.
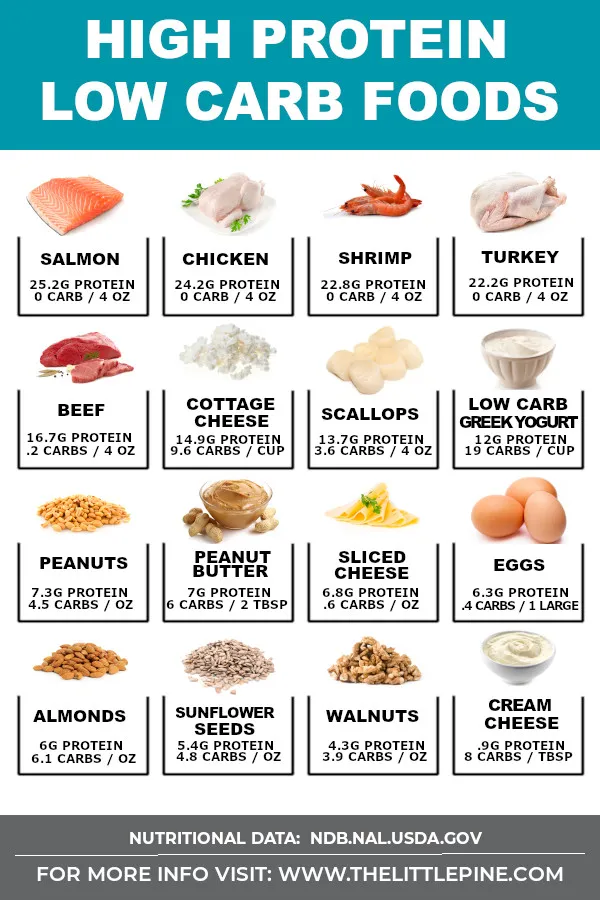
- Protein priority (roughly a quarter of the plate). Paneer, whole pulses, sprouts, legumes, eggs, or fish. Dr. Gaikwad treats protein at every major meal as non-negotiable. Higher protein intake has been found to reduce liver fat in people with NAFLD, as well as those with type 2 diabetes. Protein also preserves lean muscle mass during weight loss, which matters for long-term metabolic rate.
- Smart fat, not fear of fat. Olive oil as the primary cooking fat, with nuts, seeds, and avocado as add-ons. These displace the refined seed oils (sunflower, canola, soybean) that Dr. Gaikwad identifies as a key driver of gut and metabolic dysfunction. His clinical observation: eliminating wheat and seed oil is among the most effective interventions for resolving constipation and gut inflammation simultaneously.
- Optional carb cap. If a whole-grain source is needed, a small portion of jowar (sorghum) roti or whole pulses can be included. The key word is small. The plate's fiber and protein load should already blunt the glycemic impact of any modest carbohydrate that makes it onto the dish.
Targeting Triglycerides Specifically
High serum triglycerides are almost always a dietary signal: too much sugar and refined starch, too little fiber, not enough omega-3s. Dr. Gaikwad's science-backed triglyceride protocol calls for cutting added sugar and refined carbs first, then prioritizing healthy fats from nuts, seeds, olive oil, and avocado, eating omega-3-rich fish two to three times per week, and losing 5-10% of body weight. He also recommends 150 minutes of aerobic exercise per week, limiting alcohol, adding fiber from legumes and vegetables, staying hydrated, and protecting sleep at seven to eight hours. His summary: "Lifestyle > medicines in many cases."
This isn't a supplement stack or a pharmaceutical intervention. It's an organized removal of the inputs that force triglyceride synthesis and a replacement with inputs that support fat oxidation.
What the Patient Results Look Like
Dr. Gaikwad's clinical posts document concrete before-and-after outcomes. One patient moved from 105.5 kg to 92.5 kg, a 12% body weight drop, and research shows that even a 10-12% loss can cut liver fat by approximately 30%, improve insulin sensitivity, reduce triglycerides, and help the pancreas restart early insulin production more efficiently. In a separate case, a vegetarian patient with type 2 diabetes brought fasting blood sugar down from 150 mg/dL to 90 mg/dL in just 50 days purely through structured dietary intervention, alongside an 8 kg weight loss, improving insulin sensitivity. Neither outcome required injections, nor did either require counting net carbs to the gram. They required structure and consistency with the plate template described above.
Lab Markers to Track Over 8-12 Weeks
Following this protocol, these are the numbers worth watching on a standard metabolic panel ordered at the eight-week and twelve-week marks:
- ALT (alanine aminotransferase): The primary liver enzyme marker. Elevated ALT is a reliable proxy for hepatic inflammation and fat accumulation. Expect to see meaningful drops as liver fat clears. Clinical data shows ALT reduction correlates closely with liver fat reduction under low-carb dietary protocols.
- Serum triglycerides: The fastest-moving marker on this protocol. Cutting refined carbs often drops triglycerides within the first two to four weeks, well before body weight shifts become dramatic.
- Fasting blood glucose and HbA1c: HbA1c reflects the three-month glycemic average and is a clean signal of how effectively the plate framework is controlling post-meal glucose spikes. The CRHP dietary model has demonstrated improvements in HbA1c independent of significant weight changes.
- Waist circumference: Visceral fat, the kind packed around abdominal organs including the liver, tends to respond faster to carb reduction than subcutaneous fat. Measuring waist at the navel every two weeks is a low-tech but highly informative data point.
- Body weight trend: Not a daily weigh-in obsession, but a weekly average. The goal is a controlled 5-10% reduction over the 8-12-week window, which is the threshold at which liver fat and triglyceride improvements become clinically significant.
Putting It Together
The plate framework Dr. Gaikwad demonstrates is, at its core, a set of displacement decisions: fiber-dense vegetables displace refined grains, quality protein displaces empty-calorie snacking, olive oil and nuts displace industrial seed oils. His clinical position is direct: whether the condition is obesity, fatty liver, or diabetes, the dietary response is the same: eat more proteins and restrict carbs. You don't need to be in deep ketosis to see those lab numbers move. You need to build the plate right, repeat it consistently, and let the metabolic math do the work across two to three months of structured eating.
This article was produced by Prism’s automated news system from verified source data, official records, and press releases, then run through automated quality and moderation checks before publishing. The system is built and supervised by the people who set the standards it runs under. Read our full AI policy.
Know something we missed? Have a correction or additional information?
Submit a Tip

